Insights
5
min read
Improving Patient Collections: What Top Performers Do Differently
Most providers think their patient collections are in good shape. Top performers know there's always more on the table.
Written by
Ben Kraus
Published on
March 13, 2026
Share



Subscribe to our newsletter
Stay in the loop in our resources and insights
Thanks for your message!
We will reach back to you as soon as possible.
Patient collections is a spectrum.
There's no single right way to do it. Patient populations are made up of unique individuals whose ability to understand and pay medical bills is shaped by countless factors: where they live, how they engage with their healthcare provider, the complexity of their bill, and increasingly, the volatility of their coverage.
But across the top-performing providers we partner with, we've identified five practices that consistently set the best apart. And they don't necessarily require a full technology overhaul or a massive budget.
What they do require is a willingness to look at patient collections differently—from how you measure performance and segment accounts, to how you show up for patients at one of the most stressful moments in their healthcare experience.
What does it mean to be a top performer in patient collections?
It's tempting to answer that question with a single number. A collection rate benchmark. A cost-to-collect target. A bad debt threshold.
But high performance in patient collections isn't a single metric—and organizations that optimize for one at the expense of the others tend to find out the hard way.
A high collection rate means little if it's driven by aggressive tactics that send patients to bad debt agencies and erode trust. Low cost-to-collect is misleading if the savings are offset by patient revenue being written off. And patient satisfaction scores can look fine—until you look at what those same patients actually paid.
True top performers optimize across three dimensions simultaneously: collecting more of what’s owed, spending less to do it, and strengthening—not straining—the patient relationship.
Here's what the best do differently.
Five things top performers do differently to improve patient collections
1. Measure what really matters
You can't improve what you don't measure. While revenue cycle management is among the most measurable provider functions—with payer and AR metrics deeply embedded in operations—there is one glaring blind spot: patient collections.
It’s not for lack of trying. The systems most organizations rely on were built to track insurance reimbursement, not patient experience. And those are very different problems.
Consider one Epic-based health system that appeared to be doing everything right. Major EHR upgrade? Complete. EHR accolades for feature adoption? Earned. High patient portal activation? Check. Patient cash up 8% in one year? Impressive.
Many health systems would've stopped there. But this one wanted to go further.
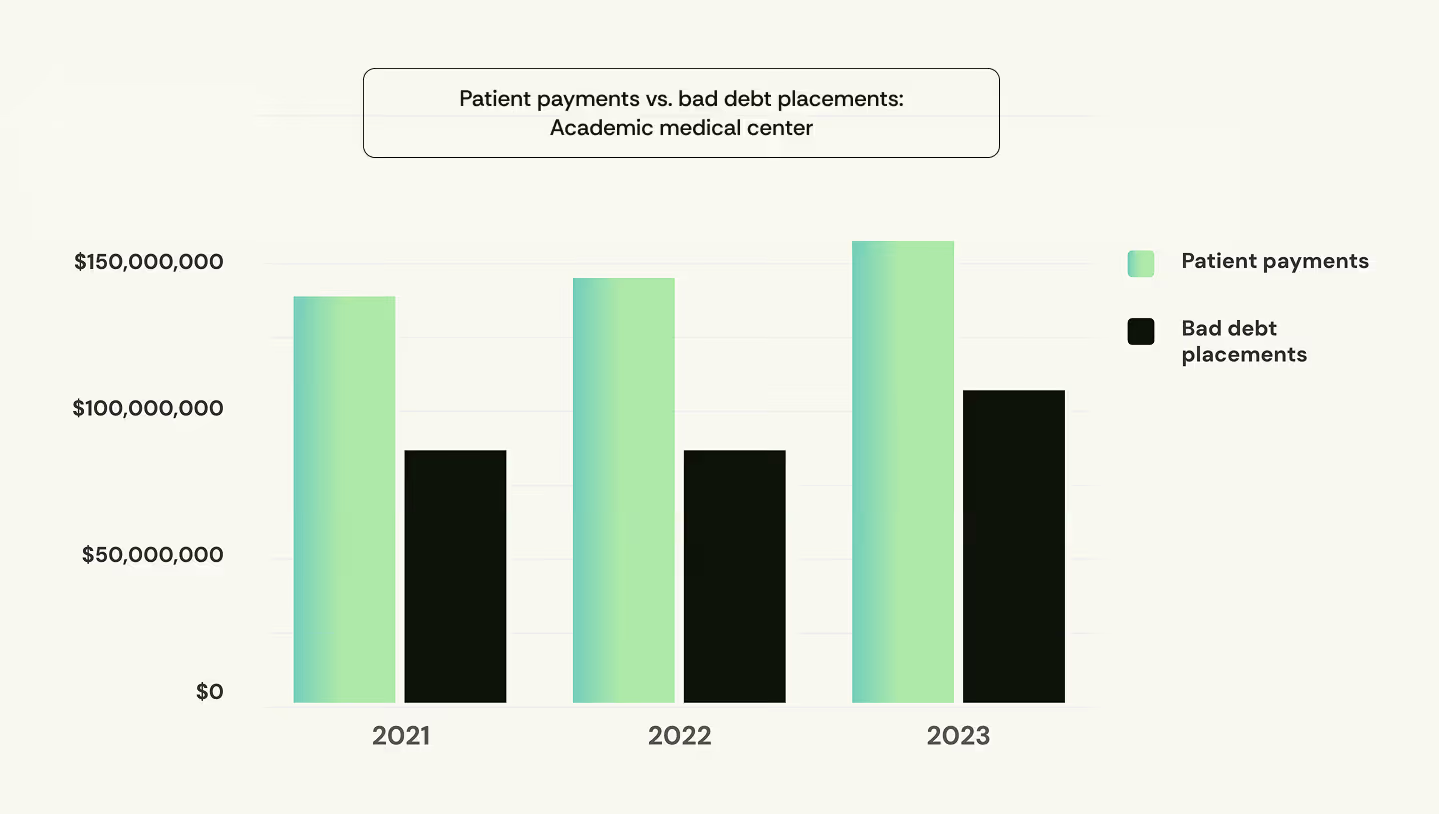
A deeper analysis revealed that bad debt placements were increasing alongside cash. Despite optimizing their EHR, 10% of total patient payments were coming from bad debt agencies—3x higher than what we typically see.
Taking a closer look, they found patient billed amounts had increased 22% over the same period. Cash was up largely because of higher volumes, not improved performance on patient receivables.
The organizations consistently outperforming on patient collections layer in a second tier of measurement alongside traditional KPIs. They track payment plan enrollment and recovery rates in addition to AR days. They monitor dollars collected through digital channels rather than just portal logins.
These signals surface where patient financial risk is building, and importantly, how to intervene before it escalates.
For a deeper look, check out our complete guide to patient financial metrics.
2. Rethink patient segmentation
Imagine a patient who was on Medicaid last week. This week, they're on a marketplace plan with a $5,000 deductible.
Would you consider that account "commercial" business, with the same capacity to pay as a patient on a fully-funded employer plan?
Probably not. Yet that's exactly how most reporting still segments patient AR, and decides which billing communications to send.
Traditional AR buckets—government, commercial, self-pay—describe insurance coverage, not patient behavior. They don't tell you someone’s financial capacity or what kind of support would help them resolve their balance. And in an environment where a growing share of commercially insured patients carry deductibles that rival what uninsured patients often owe, that gap has real consequences.
Top performers take a more nuanced approach, layering insurance status with objective, non-discriminatory behavioral and engagement data to predict payment behavior and tailor outreach accordingly.
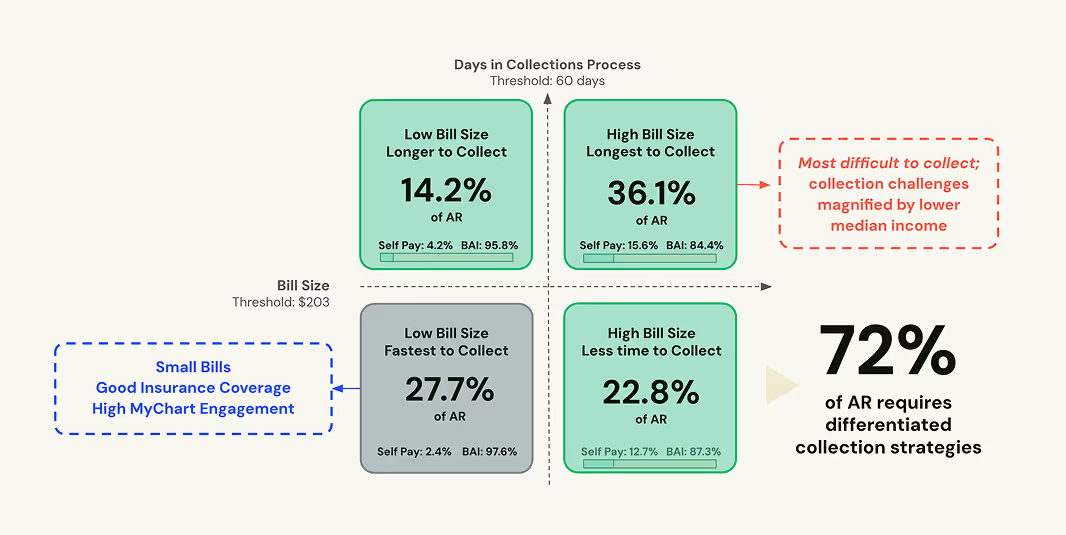
For example: when we map patient AR by bill size and days outstanding across our platform, just 28% of collectible dollars fall into the "fast and easy" bucket. These are patients with small copays who are already digitally engaged. The remaining 72% represents harder-to-collect dollars tied to patients who are underinsured, uninsured, or disengaged from the billing process entirely.
But there's more to the story. Local market conditions, prior payment behavior, and patient sentiment can all shape how (and whether) they engage. Leading organizations keep refining cohorts until outreach, payment options, and communication align with each population's actual situation.
3. Optimize staffing and vendor strategy
Segmenting the harder-to-collect dollars tells you where attention is needed. Recovering them is a different challenge entirely—and it's very much a numbers game.
Say you have 1,500 patient accounts. EHR digital billing tools handle 800 of them, the “fast and easy” dollars. Your in-house team works through another 400. That leaves 300 accounts untouched. And those 300? They represent the bulk of out-of-pocket dollars most at risk of becoming bad debt.
Closing that gap requires persistent, personalized outreach. Scaling in-house can be effective, but the costs add up: staffing, training, turnover, and the drag of managing manual processes across a constantly shifting patient population.
Top-performing organizations treat vendor strategy as a force multiplier, not a fallback. Beyond cost considerations, the vendor question has two parts:
- Can a specialized partner actually reach those harder-to-collect accounts—the 300 that would otherwise go untouched?
- How do they show up when they get there? At this point in the journey, vendors are touching patients at one of the most stressful moments in their healthcare experience. How they communicate, what options they offer, how they handle complexity—that ultimately reflects on your organization, not theirs.
The right partners treat both as non-negotiable.
And none of this is to say cost doesn't matter. It does—especially in an environment where the average hospital operates on a 2% margin.
But it's worth asking where those costs come from. Traditional early-out and bad debt vendors, for example, are built around ever-growing teams of people. That labor expense doesn’t disappear. It ultimately gets passed to providers in the form of fees and placement rates.
Top performers ask a different question: not just how to reach more accounts in a patient-friendly way, but how to change the economics of doing so.
4. Test, optimize, and repeat
There's no silver bullet in patient collections. No single feature, channel, or workflow that works for every patient, every balance, every situation.
That might seem obvious, but it's easy to lose sight of when a vendor is demoing text-to-pay and Apple Pay integrations. Those tools are genuinely useful. But imagine offering a seamless mobile payment experience to a patient staring down a four-figure emergency room bill they didn't expect. Or a patient who hasn't opened a single statement because they don't trust the bill to begin with.
Convenience isn't the barrier. Something else is.
The organizations meaningfully improving patient collections aren't searching for the right feature set. They're mapping the engagement funnel—understanding exactly where patients drop off, and designing targeted interventions for each point in the journey.

That means asking different questions at each stage. Why are certain cohorts opening text reminders but not clicking through? Why are patients getting to the checkout page but abandoning their carts? Why does outreach that works for one segment fall flat for another? The answers aren't universal—and neither are the solutions.
What separates top performers is the discipline to keep asking. They run structured tests across outreach timing, channel sequencing, message framing, and payment option design. They measure against the metrics that matter. And they use what they learn to refine the next intervention.
5. Personalize at scale with AI
The first four practices give you the right foundation. Measurement tells you where to look. Segmentation tells you who needs what. Vendor strategy ensures you can reach them. Testing tells you what works.
But they share a common constraint: they're only as dynamic as the rules you build into them.
AI shifts that equation. Machine learning models trained on patient interactions at scale don't just execute a strategy. They continually learn and improve it. Every payment made or reminder clicked or support call resolved adds to what the system knows. Over time, the model gets better at predicting what a patient needs, how they prefer to engage, and what will actually move them to resolve their balance.
That matters most for the patients who are hardest to serve. The ones whose coverage changes mid-year. The ones managing multiple bills across multiple providers. The ones whose situation might look similar on paper to a patient who paid quickly—but whose experience requires something meaningfully different.
Static rules can't account for that level of nuance at scale. AI can.
The goal isn't automation for its own sake. It's a patient financial experience that adapts as your population evolves—getting more precise with every interaction, without requiring your team to manually rethink the strategy each time.
That's the compounding advantage top performers are building. And it's the hardest one to replicate.
Frequently asked questions
1. How do we know if our current patient collection rate is actually good?
Short answer: you might be asking the wrong question.
There's no universal benchmark for a "good" patient collection rate. Rates vary significantly based on payer mix, geography, service line, and patient population—and the methodologies used to calculate them vary just as much.
More important than hitting a benchmark is measuring consistently, using a methodology that reflects how your operation actually works. The approach we've found most reliable: posted post-visit payments divided by first statement amounts, aggregated over a rolling 12-month period to account for seasonal fluctuations. It gives you a stable baseline to trend against over time.
The question worth asking isn't "is our rate good?" It's "are we getting better?" Consistent measurement with the right methodology is what lets you answer that.
2. We have limited IT resources and budget. What should we focus on first?
The most common mistake resource-constrained organizations make is investing in new capabilities before understanding where existing ones are falling short.
Before thinking about new tools or vendors, get clarity on where your current performance actually stands. Pull your first-billed collection rate alongside your account-close rate. Look at payment plan enrollment versus completion. Track digital payment conversion, not just portal logins. These signals should exist in your current reporting environment, they just aren't always being surfaced.
From there, map where patients are dropping off. If patients are viewing payment plan options but not enrolling, the issue may be that your financial policies aren't aligned with what patients can actually afford. If patients aren't engaging with text reminders, the issue may be channel fit—some populations respond better to paper statements or a different outreach cadence.
The point is to let the data tell you where to focus before spending anything. Most organizations that do this find one or two high-impact drop-off points that can be addressed without a major investment, creating the business case for bigger changes down the road.
3. We use [enter your EHR here]. Can we implement these best practices within our existing workflow?
For organizations with strong IT resources and mature data capabilities, most EHRs can be configured to support many of these practices. Segmentation logic, outreach rules, payment plan parameters—a lot is possible within the platform if you have the technical capacity to build and maintain it.
But configuration is only part of the challenge. The harder part is the operational expertise required to drive continuous optimization, such as knowing which cohorts to test, how to read drop-off signals, when to adjust outreach cadence, and how to translate data into interventions that actually move the needle. That capability doesn't come out of the box with any EHR.
There's also a patient population that EHR digital-first payment workflows simply won't reach. Some patients won't engage with a portal notification or a text reminder regardless of how well it's designed. For those patients—often the hardest-to-collect accounts—multi-modal outreach, including voice, becomes essential.
The best implementations we see use the EHR as the foundation and layer in the engagement expertise and outreach capabilities needed to reach the full patient population, not just the digitally engaged ones.
4. How do we get leadership buy-in to change how we approach patient collections?
Leadership buy-in conversations around patient collections tend to stall in the same places. We're already doing well—we have the latest EHR billing functionality. There are more pressing problems to solve—payer denials, prior auth, staffing. And any investment in this area needs to clear a high bar.
These are reasonable objections. The mistake is accepting them as conclusions rather than starting points.
The most effective case for change isn't just more data. It's also presenting trade-offs.
If we hold off, here's the cash at risk or patients falling through the cracks. If we act on what we know to be true today, here's what we can secure while continuing to refine.
That shifts the question from "are we sure enough?" to "what are we willing to leave on the table?" Most executives respond differently to the second question.
The bottom line
Every account in your AR represents a patient who came to you for care. What happens next in the billing process shapes whether they come back.
The organizations pulling ahead on patient collections aren't winning because they've found a better way to extract money. They're leading because they've built experiences that meet patients where they actually are—with the right information, the right options, and the right support at the right time.
That's what the five practices in this post are really about. Not optimizing a revenue cycle function, but closing the gap between what patients need and what the financial experience actually delivers.
The three goals—collecting more, spending less to do it, and serving patients better—aren't in tension. For top performers, they're the same goal.
See related blog posts
See how Cedar connects the dots

with an empathetic, easy-to-understand billing experience.
cost-to-collect
with self-service solutions and fewer vendors to manage.
satisfaction
with transparent billing and flexible payment options.
with agile, streamlined tools that mirror the patient’s view.


