Insights
5
min read
Cohorting Patient AR: Why 72% Need Specialized Collection Strategies
Imagine a patient who was on Medicaid last week. This week, they’re on a marketplace plan with a $15,000 deductible.Would you treat that account as “c...
Written by
Ben Kraus
Published on
November 3, 2025
Share



Subscribe to our newsletter
Stay in the loop in our resources and insights
Thanks for your message!
We will reach back to you as soon as possible.
Imagine a patient who was on Medicaid last week. This week, they’re on a marketplace plan with a $15,000 deductible.
Would you treat that account as “commercial,” with the same ability to pay as a traditionally insured patient?
Probably not. Yet that’s exactly how most providers still segment patient accounts receivable (AR) and decide which billing communications to send.
The old categories of commercial, government, and self-pay are anachronistic. They don’t just fail to predict payment behavior. They actively distort it, resulting in missed payments, wasted effort, and unnecessary friction for patients.
What providers need instead is a way to understand what each patient actually needs and route them to the right support at the right time.
Why Cohorting Patient AR Matters More Than Ever
Patient out-of-pocket costs have been climbing for years, most notably driven by the proliferation of high-deductible health plans (230% growth in spending since 2010). Patients enroll in plans that on the face of it seem affordable with lower premiums, only to get hit with a high bill when they land in the emergency room or get diagnosed with a new illness or condition.
For finance and revenue cycle leaders, this is nothing new. But the trend is accelerating.
Pandemic-era ACA subsidies expired at the end of 2025—subsidies that had doubled marketplace enrollment and made coverage affordable for more than 20 million Americans. Without them, premiums have risen sharply. As a result, 1 in 4 Americans say they’d drop coverage, leaving a smaller, sicker risk pool that drives costs even higher.
Meanwhile, Medicaid reforms are projected to strip coverage from millions more. Many will cycle between uninsurance and marketplace plans with high deductibles—exactly the patient described in the opening. They move from one coverage type to another in a matter of weeks, but their ability to pay a $10,000 medical bill remains unchanged.
And employer-sponsored insurance isn’t insulated from these dynamics. As marketplace instability increases uncompensated care, providers pass those costs through to commercial payers. The average family plan now costs just under $27,000 a year—up 6% from the prior year, continuing a trend of increases that outpace inflation.
The result: insurance status is becoming less and less predictive of payment capacity across the entire patient mix.
Four Patient Cohorts That Capture Payment Needs
If insurance doesn’t predict payment behavior, what does?
At Cedar, we’ve found that two seemingly simple dimensions can tell you a lot more about your patients: bill size and how long balances have been outstanding.1

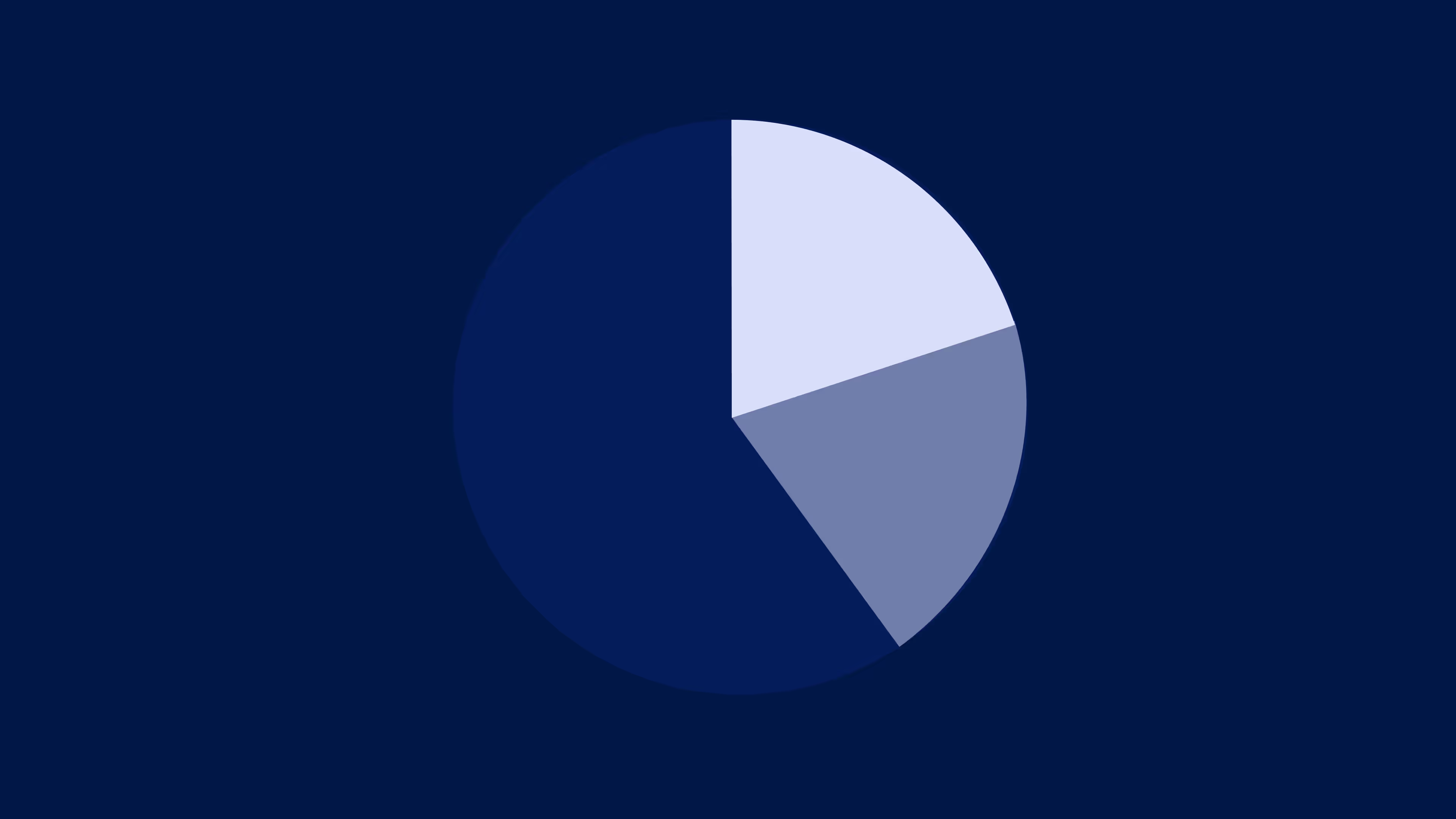
When you plot patients across these two dimensions, a pattern emerges. Applied to one large health system client, only 28% of patient dollars fall into the “fast and easy” category—digitally engaged patients with good insurance and manageable bills. These are your $20 copays, patients who pay online within 30 days.
That means 72% require specialized collection strategies.
But the traditional approach sends all of these patients the same statement, the same patient portal notification, the same follow-up cadence. Someone with a $20 copay has fundamentally different needs than someone facing a $10,000 emergency room bill.
Here’s what each segment actually needs:
1. Low Bills, Fast to Collect (28%)
What they need: Convenience and zero friction. A payment experience that matches what they get from leading consumer brands like Amazon—fast, seamless, and intuitive. Tools like Apple Pay, text-to-pay, and guest checkout deliver exactly that.
The good news: Chances are you’re already serving this segment well—this is where EHR patient financial experience tools and patient payment point solutions really shine. In fact, Cedar’s research found that 77% of consumers say that their provider offers convenient payment methods.
2. Low Bills, Longer to Collect (14%)
Who they are: These patients face competing financial priorities: multiple medical bills across different providers while juggling everyday expenses. Many are ALICE households (Asset Limited, Income Constrained, Employed), who earn above the Federal Poverty Level but not enough to make ends meet.
Here’s the key: research shows they’re highly motivated to meet their financial obligations.
What they need: Payment plans, but only if they offer the right options. Our research found that nearly half of patients (47%) can afford payments under $100 per month. Micro-payment plans that match their cash flow reality make the difference between a paid balance and a write-off.
They also need more time. Extended dunning cycles give patients room to save without forcing impossible tradeoffs elsewhere in their budget. This isn’t about being lenient. It’s about being realistic about how these patients actually manage their finances.
3. High Bills, Moderate Time to Collect (23%)
Who they are: These are typically patients on high-deductible health plans or those who received elective procedures not covered by insurance. Faster collection velocity indicates they have the means to pay.
Many have a health savings account (HSA) or flexible spending account (FSA) but don’t realize they have available funds.
What they need: Reminders that they have money that’s already earmarked for medical expenses. That means easy access to the $123 billion sitting idle in HSAs and proactive nudges to use FSA funds before they expire—especially since half of accountholders see this happen each year.
But first, make sure they should be paying at all. Coverage verification and denials resolution, including Coordination of Benefits (COB) issues, can catch what insurance should have covered before asking patients to tap their own accounts.
4. High Bills, Longest to Collect (34%)
Who they are: These patients face the most complex situations: potentially uninsured, maybe stuck in denial loops, or in the midst of health crises that have derailed their finances. For this cohort, it’s not about creating a better billing experience. They need tailored affordability solutions.
What they need: Navigation to resources that they don’t know exist. For example, pharmaceutical manufacturers fund $5 billion in patient assistance programs annually. Yet a staggering 97% of eligible patients aren’t using this benefit.
This cohort also needs automated Medicaid enrollment support (17% of eligible adults churn out due to procedural barriers), charity care screening and application assistance, third-party financing options. This requires the most intensive support, but also represents the biggest opportunity to convert write-offs into payments.
Building Truly Matched Cohorts
These four segments are just the starting point. When you layer in additional patient behavior and engagement signals, you can build out more and more micro-segments that enable increasingly precise outreach.
The goal is to continue breaking down these segments into smaller and smaller cohorts until you get to truly matched populations that you can respond to and support in tailored ways.
It’s a pretty far departure from commercial, government, and self-pay. But as the lines between coverage types and payment capacity blur, providers need a cohorting strategy that reflects what actually matters: what patients need to resolve their bill.
From transaction to navigation
For decades, patient financial experience was transactional: send a statement, wait for payment, follow up if overdue. This assumes patients can and will pay, treating every obligation the same. But when that patient who used to be on Medicaid has to pay their deductible after a visit to the ER, giving them the option to pay with Apple Pay isn’t just irrelevant. It’s absurd.
Put bluntly, providers have perfected the art of asking patients to pay bills they can’t afford. The next step is helping them navigate the resources that exist but are scattered across the healthcare ecosystem and disconnected from the patient experience.
The new model works like GPS. Instead of handing every patient the same map, it reroutes based on their actual situation, anticipates obstacles, and guides them to the most relevant solutions. That means intelligently connecting patients to the right resources and options at the right moment.
Now more than ever, patients are weighing affordability at every turn, deciding whether to access care, skip a dose, or delay treatment. The question for providers is simple: what if affordability were the starting point for every patient interaction, not something to react to after the bill is sent?
Ben Kraus is Director, Content Marketing at Cedar
- This cohorting approach primarily reflects engagement and billing complexity, and is designed to comply with applicable law. It is intended to help providers provide support where it’s needed most, improving both collections and the patient experience ↩︎
See related blog posts

Built for patients. Powered by intelligence. Proven in performance.
Product visuals and descriptions may be in development and are subject to change. Certain functionalities may require third-party integrations or service-specific terms or fees. Patients served, patient interactions, and payments processes represent Cedar cumulative metrics since 2017. Cedar Support, Cedar Kora, and Cedar Cover metrics reference data from pilots in 2024 and 2025. Cedar Pay metrics reference data from 2023 to 2026, including weighted averages. All performance metrics, as well as testimonials from Cedar clients, are provided solely for illustrative purposes, and are not a guarantee of future results.
